Micro-specialisation and prognosis overestimation
I am a general dental practitioner, a jack-of-all trades in the dental world and possibly becoming an endangered species. To keep updated I travel to a lot of international conferences that cover the dental disciplines such as implants, restorative dentistry, prosthetics, endodontics, and periodontics to name a few. To my mind dentistry is a speciality within general healthcare so the disciplines above should be considered as sub-specialities or micro-specialities of dentistry and over recent years there has been a shift away from the generalist to the specialist (1). What I observed was that each discipline is just a bit better than the other at saving or restoring teeth so at an implant based conference implants outperform root-fillings and vice-versa. Now if one carefully adds up the success rates across the disciplines of all the treatment options it becomes greater than 100%, which it impossible. What is happening is, due to uncertainty the clinicians have to use probabilistic data and by restricting the number of treatment options create overestimates for the relative success or suitability of that treatment. This is a problem of ‘subadditivity’ and the ‘unpacking principle’:
Subadditivity – This is where the sum of two probabilities is greater than 1.0.
Unpacking – As more detail of a hypothesis is provided (unpacked) there is an increase in its estimated probability.
An EBSCO literature search using the search terms “unpacking principle or subaddition” and “medical decision making” produced three relevant papers with no systematic reviews or meta-analysis(2–4).To summarise the results; in Cahan et al’s paper 65% of the doctors exhibited subadditivity with a mean probability of 137% and Redelmeier et al concluded that clinicians need to unpack a broad category of treatment opptions rather than compare a single treatment against unspecified options.
To help understand these concepts I have worked an example for you below:
“A patient attends a dental surgeon complaining of difficulty chewing due to a loss of lower back teeth. On one side are two premolars and on the other one premolar. Both last standing teeth need new crowns. The upper arch is intact.”
The option are as follows:
- No treatment ( I will ignore this options in this example.)
- Two milled crowns and a metal/acrylic denture.
- Two crowns and a single implant following the shortened arch concept(5).
- Two crowns and four single implants. (Maximised model)
- Two tooth-implant retained three unit bridges (F-I).
The 10-year survival estimates for the individual components of the above treatment are:
- Single metal-ceramic crown 94% (6).
- Single tooth implant 89% (7)
- Tooth-implant bridge 77% (7)
- Metal acrylic denture 50% (8)
Looking at the individual survival figures the best treatment options involve metal-ceramic crowns on vital teeth or single crown implants, the next option is the tooth-implant bridge and finally the denture. The intuitive choice of most people would be Option 4. (Two crowns and four single implants) due to the high survival rates. Once one becomes aware of the effects of subaddition and unpacking however Option 4. is not such a strong option as it at first appears in terms of complications and maintenance costs (Table 1.)
| Unit treatment option | 10-year Survival | P | Complete Treatment options | Options | Complication free | |
| Implant Single crown (SCI) | 89 | 0.89 | 2 crowns ,1 implant | 2 x SC,1x SCI | 0.79 | |
| Single crown (SC) | 94 | 0.94 | 2 crowns, I denture | 2 x SC, Co/Cr | 0.44 | |
| Cobalt chrome denture (Co/Cr P) | 50 | 0.5 | 2 crowns,4 implants | 2 x SC, 4 x SCI | 0.55 | |
| Fixed-implant bridge (F-I) | 70 | 0.7 | 2 Fixed-Implant bridges | 2 x F-I | 0.49 |
Table 1.
The avoid the cognitive error of subaddition the clinician/patient can only choose one option to follow, this is best represented as a pie-chart (Fig 1.).
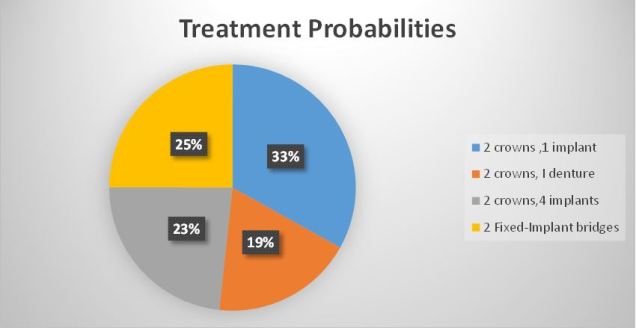
Fig 1.
The conclusion when the treatment options are unpacked and compared is that the two bridges or the two crowns/four implants have about the same complication rate. The two crowns and the implant is the safest and the denture option has the highest failure rate.
There is however one more consideration and that is relative cost/benefit which is generally overlooked in the research literature. Fortunately, with the data above it is quite simple to calculate this using the concept of ‘expected value’ For this example I have used the total estimated cost of the treatment and multiplied it by the probability of a complication. To calculate the probability of any complication I used the formula (Table 2):
p(complication)=1-p(complication-free).
| Treatment options | Options | Complication free | Complications (P) | Estimated Treatment Cost | Estimated Value |
| 2 crowns ,1 implant | 2 x SC,1x SCI | 0.79 | 0.21 | 3700 | 790 |
| 2 crowns, I denture | 2 x SC, Co/Cr | 0.44 | 0.56 | 2200 | 1228 |
| 2 crowns,4 implants | 2 x SC, 4 x SCI | 0.55 | 0.45 | 11200 | 4991 |
| 2 Fixed-Implant bridges | 2 x F-I | 0.59 | 0.41 | 6000 | 2443 |
Table 2.

Fig 2.
Hopefully it’s clear that initially the two crown, four implant option may be more appealing it does carry a significantly greater cost compared to the bridges. The safest treatment both in terms of cost and predictability is the shortened arch principle due to its simplicity.
The ‘take-home message’ is that as the number of treatment items increase for an individual, the risk of complications and cost can also increase. By taking a little time to ‘unpack’ the alternate treatment options it can help reduce overconfidence and clarify choice as part of the consent process.
References:
- Levin-Scherz J. What Drives High Health Care Costs. Harv Bus Rev [Internet]. 2010;88(4):72–3. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20402058
- Redelmeier DA. Medical Decision Making in Situations That Offer Multiple Alternatives. JAMA J Am Med Assoc [Internet]. American Medical Association; 1995 Jan 25 [cited 2014 Mar 11];273(4):302. Available from: http://jama.jamanetwork.com/article.aspx?articleid=386588
- Liberman V, Tversky A, Redelmeier DA. The Psychology of Decision Making Probability Judgment in Medicine : 1995;
- Cahan A, Gilon D, Manor O, Paltiel O. Probabilistic reasoning and clinical decision-making: Do doctors overestimate diagnostic probabilities? QJM – Mon J Assoc Physicians. 2003;96(10):763–9.
- Käyser a F. Shortened dental arches and oral function. J Oral Rehabil. 1981;8(5):457–62.
- Reitemeier B, Hansel K, Kastner C, Weber A, Walter MH. A prospective 10-year study of metal ceramic single crowns and fixed dental prosthesis retainers in private practice set tings. J Prosthet Dent [Internet]. The Editorial Council of the Journal of Prosthetic Dentistry; 2013;109(3):149–55. Available from: http://dx.doi.org/10.1016/S0022-3913(13)60034-7
- PJETURSSON BE, LANG NP. Prosthetic treatment planning on the basis of scientific evidence. J Oral Rehabil [Internet]. 2008;35(s1):72–9. Available from: http://doi.wiley.com/10.1111/j.1365-2842.2007.01824.x
- Vermeulen a H, Keltjens HM, van’t Hof M a, Kayser a F. Ten-year evaluation of removable partial dentures: survival rates based on retreatment, not wearing and replacement. J Prosthet Dent [Internet]. 1996 Sep;76(3):267–72. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8887799
