A Re-analysis of Dayer et al (2014)
Abstract
Over the past twelve months there has been a substantial amount of correspondence toing and froing in the medical/dental journals with regard to the National Institute of Clinical Excellence (NICE) Guidelines on antibiotic prophylaxis for infective endocarditis (IE). In 2008 NICE recommended complete cessation of antibiotic prophylaxis for infective endocarditis. Last year saw the publication in the Lancet of an analysis of infective endocarditis incidence 2000-2013 which precipitated a review by NICE of their position. Following their review the conclusion was that the new evidence may be at a high risk of bias and held the position of complete cessation even for high risk individuals.
In this paper I have taken the data produced by Dayer et al and reprinted in Clinical Guidance 64 (PIE) Appendix O. Professor Ramsey concluded the abstracted data was robust enough for analysis so I have also take the liberty of analysing it.
The statistical analysis applied to this data by Ramsey appeared too complex for the normal general dental practitioner to comment on its validity. To this effect I have applied a simpler and more intuitive transformation commonly used in quality control called a Shewart Control Chart. From this analysis there are three observations:
- The data should not be analysed as a combined figure as the low risk population drowns the signal from the high risk.
- The introduction of the NICE policy of cessation of antibiotic prophylaxis has not altered the incidence of IE on low risk individuals.
- There is a strong signal change in the incidence numbers mid 2008 for the high risk individuals.
My independent analysis using unconventional (to the medical establishment) analytical tools concludes even allowing for an increase in IE prior to 2008 there is still a significant increase in cases in the high risk population starting in early 2008. Therefore unless there is strong evidence to the contrary NICE guidelines need to come into line with the European Society of Cardiology guidelines with immediate effect. This means giving antibiotic prophylaxis only to high risk individuals undergoing high risk procedures. Where perfect data cannot be provided then it is our duty to make best use of the data at hand and apply the principle of Occam’s razor – “Among competing hypotheses, the one with the fewest assumptions should be selected”.
Introduction
Over the past twelve months there has been a substantial amount of correspondence toing and froing in the British medical/dental journals with regard to the National Institute of Clinical Excellence (NICE) Guidelines on antibiotic prophylaxis for infective endocarditis (IE)(1,2). In 2008 NICE recommended complete cessation of antibiotic prophylaxis for infective endocarditis. This point of view is supported by both the British Dental Association(3) and the Faculty of General dental Practitioners(4). Last year saw the publication in the Lancet of an analysis of infective endocarditis incidence 2000-2013 in England(5) which precipitated a review by NICE of their position. Following their review the conclusion was that the new evidence may be at a high risk of bias and held the position of complete cessation even for high risk individuals(6).
Practitioners rely heavily on these guidelines to help formulate the best and safest treatment plans for their patients. Until the publication of the post guideline review in the Lancet there was not point of reference to assess the changes the guidelines had made. After reading the article and the subsequent comments in the NICE review there were some questions that still was not adequately answered, such as the increase in endocarditis if removing prophylaxis was not a factor? If the data was correct then what about the analysis and interpretation. The critic in the NICE review does not clarify the question as to why there is a data shift or when it occurs.
In this paper the data produced by Dayer et al was reprinted in Clinical Guidance 64 (PIE) Appendix O. Professor Ramsey concluded the abstracted data was robust enough for analysis, so this is the data set used in the analysis below.
Methods
The NICE review document provided me with the abstracted data from Dayer et al in Appendix 1. Page 476. The data from Appendix 1. Was entered into a standard Excel spreadsheet for analysis.
The data has been divided into three tables:
- High and Low Risk combined
- High Risk
- Low Risk
I cannot make any comment of the technicalities of change point analysis, segmented regression or Hinkley algorithms since I have no training in these areas.
To analyse the data I have plotted using a Shewart Individuals Control Chart(7).
The centre line is the median of the individual values to reduce the effect of outliers.
The Upper Natural Process Limit (UNPLx) based on median values of the moving range is utilised to eliminate the natural variability in the incidence values. The UNPLx is the 3 sigma limit of the time sequence. The advantages are:
- The three-sigma limits will filter out virtually all of the routine variation regardless of the shape of the histogram.
- Any data point that falls outside the three-sigma limit is a potential signal of a change
- Symmetric, three-sigma limits work with skewed data.
This data analysis is extremely simple but powerful in its transparency and ease of reproduction without complex statistical tools.
To interpret the chart there are two stopping rules.
- Two consecutive values above the UNPLx signify a signal (3 standard deviations from median).
- Eight or more successive values on the same side of the median centre line means the time series has shifted from its historic reference, the chances of this happening are over 128:1 (p=0.996)
The initial charts are using the base line date up to the implementation of the new NICE guidelines to set median and UNPLx values. The median and UNPLx values are based on the values 1-99 (Paragraph 2.1)
If the chart fulfils either of the two rules above then the incidence rate is significantly altering and the median/UNPLx values are recalculated using the eight values that are out of specification.
Results
Combined Incidence Data
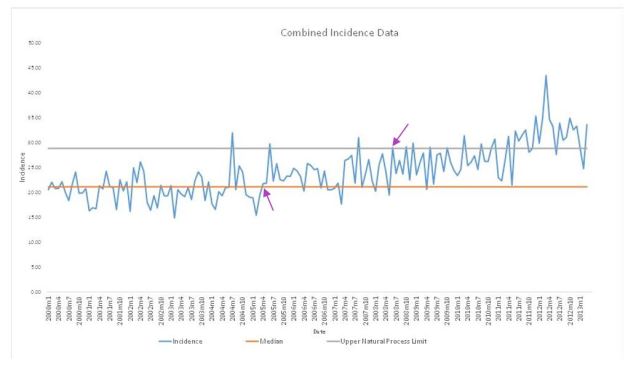
There is a signal change at 2005m4 (data point 65) and another at 2008m6 (data point 103). If I correct the median and UNPLx starting at point 65 then the second signal change still remains at June 2008 and continues to drift further away from the median from there until its two consecutive data points beyond 3 sigma at 2012m2.

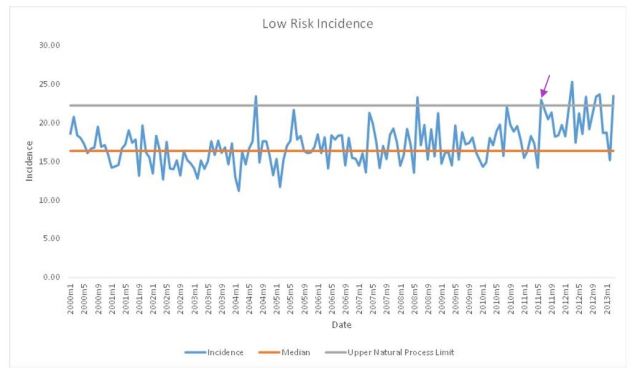
Low Risk Incidence
The low risk chart shows no signal change until 2011m6.
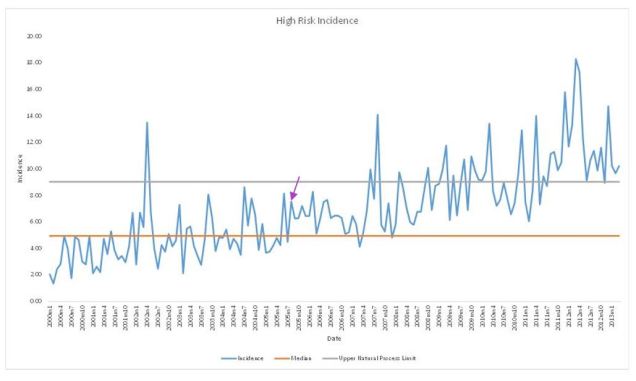
High Risk Incidence
The first signal change is at 2005m8 so the median/UNPLx was corrected upwards and the first major signal change appears on the 2008m7 and continues in an upward trend. At 2011m8 there are two consecutive data points above the 3 sigma level (UNPLx).
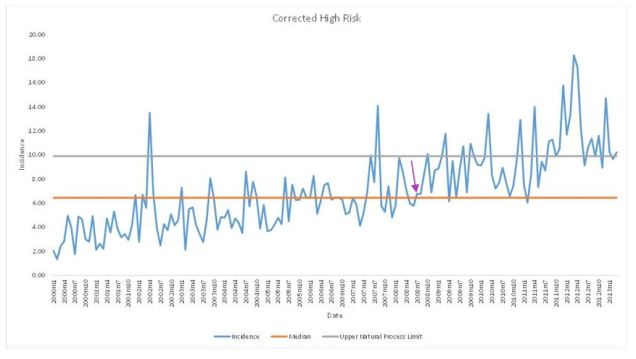
Corrected data using 2008 to 2011
If one segments the data sequence it is possible to give the illusion of hiding the signal. This is achieved by selecting the data from the guidelines change (2008m2 to 2011m4 when the time line start to shift 3 sigma from median) and recalculating the median and UNPLx. Two things to note however, the chart distinctly shows a reduced incidence before the guideline change and the single point above the UNPLx may be an outlier and need specific investigation. I placed in the lower natural process limit to show that the more variability one includes in the data the more the noise increase so only the most extreme data exceeds the control limit.

Interpretation
The NICE critique by Ramsey focused predominantly on the interpretation of the combined values chart using fairly complex modelling beyond my understanding. The answer to the question however cannot be found in the combined chart as to whether we should give antibiotic prophylaxis to high risk individuals having high risk procedures. The graph is moderately confounded by combining the low risk/high risk data within the population studied. There was a change in signal in 2005 which needs explaining but this may be due to a gradual increase in the number of high risk individuals as the population ages. Having said that, the signal alters again in June 2008, six months after the guideline implementation and continues to move out of statistical control.
Additionally by adding multiple change points in paragraph 3.2 (visualised in Figure 3) the analysis is removing the past history as it proceeds thus giving the illusion of a reduced change. This in effect hides the signal change.
The low risk chart shows no change until mid-2011 confirming that there is no data to support antibiotic prophylaxis for low risk individuals. The larger number of low risk individuals to high risk individuals dilutes the signal change in the combined graph.
The high risk chart mirrors the combined chart in showing a signal change in 2005 and when corrected still shows a change in mid-2008.
Conclusion
The Ramsey review appears to focus purely on a critique of the data analysis of the combined incidence rather than answering the question of whether the data supports continued withdrawal of antibiotic prophylaxis for high risk individuals having high risk treatments. The gradual rise in infective endocarditis incidence may be a function of a general increase of vulnerable individuals and needs further investigation so a correction factor can be applied. The data must be looked at separately and not in the combined incidence data set as the larger group of low risk cases drowns out the signal from the high risk. This may explain the increase at 2005. There is a definite signal change in the high risk individuals in 2008. The contrast between the low and high risk individuals supports the argument for reinstating AP in line with the European guidelines. Further data needs to be collected to analyse the change point in 2011, however the rule of small numbers may apply to the outliers.
References
- Chambers JB, Thornhill M, Shanson D, Prendergast B. Antibiotic prophylaxis of endocarditis: a NICE mess. Lancet Infect Dis [Internet]. Elsevier Ltd; 2016;16(3):275–6. Available from: http://linkinghub.elsevier.com/retrieve/pii/S1473309916000487
- Mohindra RK. A case of insufficient evidence equipoise: the NICE guidance on antibiotic prophylaxis for the prevention of infective endocarditis. J Med Ethics [Internet]. 2010;36(9):567–70. Available from: http://jme.bmj.com.abc.cardiff.ac.uk/content/36/9/567
- Thompson W, Palmer NOA. Guideline comment: Infective endocarditis. Nat Publ Gr [Internet]. Nature Publishing Group; 2015;219(7):303. Available from: http://dx.doi.org/10.1038/sj.bdj.2015.761
- Endocarditis I. FGDP(UK) supports NICE decision on guidance for prophylaxis against infective endocarditis. Bdj [Internet]. 2015;219(7):312–312. Available from: http://www.nature.com/doifinder/10.1038/sj.bdj.2015.789
- Dayer MJ, Jones S, Prendergast B, Baddour LM, Lockhart PB, Thornhill MH. Incidence of infective endocarditis in England, 2000-13: A secular trend, interrupted time-series analysis. Lancet [Internet]. Elsevier Ltd; 2015;385(9974):1219–28. Available from: http://dx.doi.org/10.1016/S0140-6736(14)62007-9
- Centre for Clinical Practice at NICE (UK). Prophylaxis against infective eendocarditis : antimicrobial prophylaxis against endocarditis in adults and children undergoing interventional procedures. 2015;(September).
- DJ Wheeler. Understanding variation – The Key to Managing Chaos. SPC Press; 1993.
