As a dentist I have a particular interest in how we can protect both our patients and staff during the Covid-19 pandemic and as a consequence have been closely following the development if the NHS test and trace protocols.
One of the major concerns at present is the asymptomatic carriers of the virus and the risk they pose to public health as potential super spreaders (Dental Elf – 2nd Jun. 2020). The proportion of asymptomatic test positive patients in the ONS data from July 2020 was 67% (ONS, 2020a). There are similarly high number of asymptomatics if we look at the results from Iceland at 43% (Oran and Topol, 2020).
Could this figure be correct or is it due to the high number of false positives created by a low level of infection in the community coupled with increased testing/screening (Watson et al., 2020)? There has been a push for increased screening to help unlock the community or identify hotspots, but could this screening create false hotspots because of the false-positive rate?
Method
Using the following assumptions: –
- The prevalence in England as of July was 0.05% (ONS, 2020b)
- Our testing is near perfect: sensitivity 99%, specificity 99% (Dental Elf – 12th May 2020)
- Following a local outbreak in a factory we randomly screen 5000 individuals from a large town (Population 100,000)
Figure 1. Frequency tree for Covid-19 screening
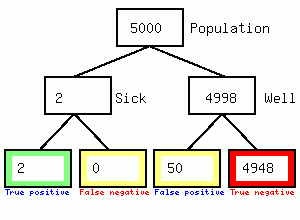 We get 2 positives and 50 false positives, so the test results is 2/52 or 3.8% accurate but the town becomes locked down causing considerable second and third order harm to the population in the form of reduced access to the hospital/GP/dental practice, and local business failures. Secondly it feeds the impression of high numbers of asymptomatic carriers since the 50 false positives will not have symptoms. I could not find any evidence that individuals having a positive swab were immediately tested again, if they were the diagnosis would be 67% accurate as shown in the following figure
We get 2 positives and 50 false positives, so the test results is 2/52 or 3.8% accurate but the town becomes locked down causing considerable second and third order harm to the population in the form of reduced access to the hospital/GP/dental practice, and local business failures. Secondly it feeds the impression of high numbers of asymptomatic carriers since the 50 false positives will not have symptoms. I could not find any evidence that individuals having a positive swab were immediately tested again, if they were the diagnosis would be 67% accurate as shown in the following figure
Figure 2. Frequency tree for repeat Covid-19 screening of positive tests
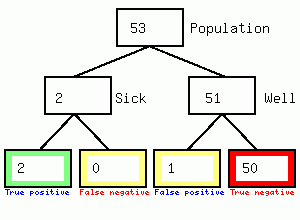
*NB. Figure of 53 is obtained because of rounding outcome data from figure 1.
Summary
- Low prevalence of Covid-19 can be problematic if governments do not understand how diagnostic tests work.
- Screening sounds like a good idea if it is backed up by an immediate second or third retest for an initial positive swab, thus allowing the false positive patients to come out of an unnecessary quarantine.
- Testing, Track and trace, self-isolating and local lock downs could be severely compromised by the false positive rates even with good testing.
References
ONS. 2020a. Coronavirus (COVID-19) Infection Survey pilot England, 24 July 2020. [Accessed 26th July].
ONS 2020b. Coronavirus (COVID-19) infections in the community in England July 2020. [Accessed 26th July].
Oran DP, Topol EJ. Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review [published online ahead of print, 2020 Jun 3]. Ann Intern Med. 2020;M20-3012. doi:10.7326/M20-3012
Watson J, Whiting PF, Brush JE. Interpreting a covid-19 test result. BMJ. 2020;369:m1808. Published 2020 May 12. doi:10.1136/bmj.m1808


